
Introduction
The alarming rise in global obesity has triggered considerable concern and has positioned it as a critical public health issue [1]. Obesity isn’t merely a matter of aesthetics; it’s intertwined with a plethora of health complications, from cardiovascular diseases to type 2 diabetes, which collectively place a substantial burden on healthcare systems [2]. In the face of this challenge, several strategies have emerged to combat obesity. Among them, surgical weight loss solutions have proven to be particularly effective for those who have had little success with traditional weight loss methods. Among the surgical options available, Gastric Bypass and Gastric Sleeve are frequently debated, both having their unique merits and challenges.
The Gastric Bypass, technically known as the Roux-en-Y Gastric Bypass, has long been regarded as the gold standard for weight loss surgery [3]. On the other hand, the Gastric Sleeve or Sleeve Gastrectomy, while relatively newer, has garnered attention due to its simpler approach and promising outcomes [4]. Both these procedures have transformative potential, but choosing between them is complex. It involves profoundly understanding each procedure’s pros and cons and aligning these with the patient’s medical history, lifestyle, and weight loss goals.
This article endeavours to compare these two prominent weight loss surgeries comprehensively. From detailing their procedures to discussing their outcomes, we aim to offer readers clarity, assisting them in making informed decisions in consultation with their healthcare providers. Additionally, considering that each patient’s journey is unique, we will emphasise the importance of personalised care and the pivotal role post-operative management plays in ensuring long-term success [5].
Gastric Bypass (Roux-en-Y Gastric Bypass)
Definition and Overview
Gastric Bypass, often termed the Roux-en-Y Gastric Bypass (RYGB), is one of the most commonly performed weight loss surgeries worldwide. This surgical procedure primarily functions by both restricting food intake and decreasing nutrient absorption, thereby inducing substantial weight loss [6].
Procedure Details
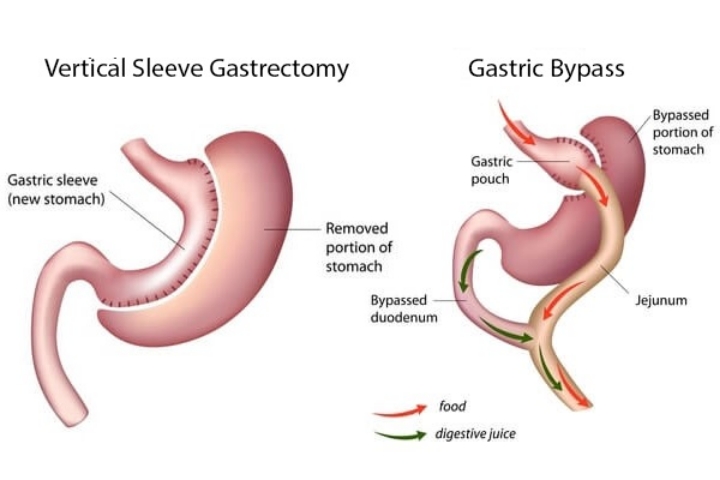
During the RYGB procedure, a small stomach pouch is created, typically holding about one ounce of food. This pouch is then directly connected to the middle portion of the small intestine, bypassing the rest of the stomach and the upper segment of the small intestine [7].
As a result, not only is the food intake limited due to the small size of the pouch, but there’s also a reduced absorption of calories and nutrients in the bypassed segment of the intestine. The procedure usually lasts 2 to 4 hours, followed by a hospital stay ranging from 2 to 5 days, depending on individual recovery rates and potential complications [8].
This dual action—restricting intake and minimising absorption—often results in more pronounced weight loss compared to surgeries that use only one of these mechanisms. Additionally, the hormonal changes post-surgery often improve weight-related health issues, such as type 2 diabetes [9].
Gastric Sleeve (Sleeve Gastrectomy)
Definition and Overview
The Gastric Sleeve, medically referred to as Sleeve Gastrectomy, stands as a popular weight loss surgical option. Unlike Gastric Bypass, the Gastric Sleeve procedure operates predominantly on the principle of restricting food intake without altering the food’s pathway through the digestive tract [10]. During the surgery, a significant portion (about 75-80%) of the stomach is removed, leaving behind a tubular or “sleeve-like” pouch.
Procedure Details
The Sleeve Gastrectomy is a laparoscopic procedure where surgeons remove the curved part of the stomach, which significantly reduces its volume. This limits the amount of food one can consume and leads to hormonal changes that can suppress appetite. One notable hormone affected is ghrelin, often termed the “hunger hormone”, which sees a notable reduction post-surgery, thereby decreasing hunger [11].
The surgery typically takes between 1 to 2 hours, with patients usually spending 2 to 3 days in the hospital for post-operative recovery. While the procedure is irreversible, it’s touted for its relative simplicity and lower complication rate compared to more complex bariatric surgeries [12].
Although Gastric Sleeve doesn’t directly interfere with nutrient absorption, patients may still require vitamin and mineral supplementation, and regular follow-ups ensure nutritional adequacy and monitor potential complications like reflux [13].
Direct Comparison Between Gastric Bypass and Gastric Sleeve
Weight Loss Expectations
While both Gastric Bypass (RYGB) and Gastric Sleeve result in significant weight loss, the degree and duration of weight loss might differ. RYGB typically results in slightly greater weight loss, with patients losing, on average, 60-80% of their excess body weight within the first 12-18 months post-surgery [14]. In contrast, Gastric Sleeve patients usually experience a loss of 50-70% of their excess body weight in the same timeframe [15].
Duration of Hospital Stay and Recovery Time
Both surgeries require hospitalisation, but their durations differ marginally. Patients undergoing RYGB generally need a hospital stay of 2 to 5 days, while those opting for Gastric Sleeve typically spend 2 to 3 days [16]. Recovery times also vary slightly, with most RYGB patients resuming normal activities within 3 to 5 weeks and Gastric Sleeve patients within 2 to 4 weeks.
Complication Rates
Both procedures have their risks. However, due to the rerouting of the digestive tract in RYGB, there’s a slightly increased risk of nutritional deficiencies and dumping syndrome. In this condition, food moves too quickly into the small intestine [17]. Gastric Sleeve, while generally having fewer complications, might increase the risk of acid reflux or heartburn [18].
Impact on Comorbidities
Both surgeries significantly improve or even resolve obesity-related comorbidities, including type 2 diabetes, hypertension, and sleep apnea. RYGB, however, often has a more pronounced effect on diabetes remission due to the profound hormonal changes it induces [19].

Factors to Consider When Choosing a Procedure
Individual Health Concerns
When evaluating the best surgical option, weighing individual health concerns is imperative. For instance, patients with severe gastroesophageal reflux disease (GERD) might fare better with a RYGB, which can often alleviate these symptoms [20]. Conversely, those with a history of Crohn’s disease or certain other gastrointestinal conditions may be better suited for the Gastric Sleeve [21].
Desired Weight Loss and Maintenance
While both procedures yield substantial weight loss, RYGB generally results in slightly more pronounced reductions and may be more effective for those seeking the highest possible weight loss percentages [22]. Gastric Sleeve, however, offers a less complicated procedure, which some might prefer, especially if they are targeting moderate weight loss.
Lifestyle and Dietary Habits
Post-operative dietary habits vary between the two surgeries. RYGB patients might experience dumping syndrome if they consume sugary or high-fat foods, necessitating stricter dietary discipline [23]. Gastric Sleeve patients have fewer dietary restrictions but might be more prone to acid reflux, especially when consuming spicy or acidic foods [24].
Concerns About Nutritional Deficiencies
Given the bypass of a segment of the small intestine in RYGB, there’s an increased risk of nutritional deficiencies, necessitating lifelong supplements [25]. Though Gastric Sleeve patients can also face deficiencies, the risk is generally lower due to the preservation of the natural digestive pathway.
Conclusion
Choosing between a Gastric Bypass and a Gastric Sleeve is a pivotal decision that hinges on individualised health concerns, weight loss goals, lifestyle considerations, and potential side effects.
While RYGB boasts a slightly more significant weight loss potential and can be particularly effective for conditions like GERD [26], the Gastric Sleeve offers a simpler surgical approach with fewer potential nutritional deficiencies and a relatively uncomplicated post-operative lifestyle [4]. It’s essential to acknowledge that there’s no one-size-fits-all answer in bariatric surgery. Both surgeries have transformed countless lives, instigating substantial weight loss and remarkable improvements in obesity-related comorbidities [27].
Collaborative decision-making, involving a comprehensive discussion with a bariatric surgeon and multidisciplinary team, will ensure that the chosen procedure aligns with the patient’s unique needs and long-term goals [16]. Regardless of the choice, long-term success requires commitment to post-operative dietary, lifestyle modifications, and regular medical follow-ups [28].
References
- World Health Organization. “Obesity and overweight.” (2018).
- Guh, D. P., et al. “The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis.” *BMC public health* 9.1 (2009): 88.
- Buchwald, H., et al. “Bariatric surgery: a systematic review and meta-analysis.” *JAMA* 292.14 (2004): 1724-1737.
- Rosenthal, R. J., et al. “International Sleeve Gastrectomy Expert Panel Consensus Statement: best practice guidelines based on experience of>12,000 cases.” *Surgery for Obesity and Related Diseases* 8.1 (2012): 8-19.
- Courcoulas, A. P., et al. “Surgical Treatments and Outcomes of Patients with Obesity and Cardiovascular Disease.” *Circulation* 140.16 (2019): 1363-1372.
- Chang, S. H., et al. “The effectiveness and risks of bariatric surgery: an updated systematic review and meta-analysis, 2003-2012.” *JAMA surgery* 149.3 (2014): 275-287.
- English, W. J., et al. “American Society for Metabolic and Bariatric Surgery estimation of metabolic and bariatric procedures performed in the United States in 2016.” *Surgery for Obesity and Related Diseases* 14.3 (2018): 259-263.
- Sjöström, L. “Review of the key results from the Swedish Obese Subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery.” *Journal of internal medicine* 273.3 (2013): 219-234.
- Schauer, P. R., et al. “Bariatric surgery versus intensive medical therapy for diabetes—5-year outcomes.” *New England Journal of Medicine* 376.7 (2017): 641-651.
- Peterli, R., et al. “Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity: The SM-BOSS randomized clinical trial.” *JAMA* 319.3 (2018): 255-265.
- Cummings, D. E., et al. “Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery.” *New England Journal of Medicine* 346.21 (2002): 1623-1630.
- Gagner, M., et al. “The Second International Consensus Summit for Sleeve Gastrectomy, March 19–21, 2009.” *Surgery for Obesity and Related Diseases* 5.4 (2009): 476-485.
- Major, P., et al. “Nutritional deficiencies following sleeve gastrectomy: An update.” *Obesity Surgery* 28.2 (2018): 313-324.
- Adams, T. D., et al. “Weight and metabolic outcomes 12 years after gastric bypass.” *New England Journal of Medicine* 377.12 (2017): 1143-1155.
- Salminen, P., et al. “Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss at 5 Years Among Patients With Morbid Obesity: The SLEEVEPASS Randomized Clinical Trial.” *JAMA* 319.3 (2018): 241-254.
- Brethauer, S. A., et al. “Standardized outcomes reporting in metabolic and bariatric surgery.” *Surgery for Obesity and Related Diseases* 11.3 (2015): 489-506.
- Tack, J., et al. “Dumping syndrome after esophageal, gastric or bariatric surgery: pathophysiology, diagnosis, and management.” *Obesity Reviews* 18.1 (2017): 68-85.
- Daes, J., et al. “Laparoscopic sleeve gastrectomy: symptoms of gastroesophageal reflux can be reduced by changes in surgical technique.” *Obesity Surgery* 22.12 (2012): 1874-1879.
- Mingrone, G., et al. “Bariatric–metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial.” *The Lancet* 386.9997 (2015): 964-973.
- Himpens, J., et al. “Long-term results of laparoscopic Roux-en-Y Gastric bypass: evaluation after 9 years.” *Obesity Surgery* 22.10 (2012): 1586-1593.
- Colquitt, J. L., et al. “Surgery for weight loss in adults.” *Cochrane Database of Systematic Reviews* 8 (2014).
- Karmali, S., et al. “Bariatric surgery: a primer.” *Canadian Family Physician* 56.9 (2010): 873-879.
- Kellogg, T. A. “Dumping syndrome after gastric bypass: a review.” *Current Gastroenterology Reports* 11.5 (2009): 417-422.
- Melissas, J., et al. “Sleeve gastrectomy-a restrictive procedure?” *Obesity Surgery* 18.1 (2008): 57-62.
- Aills, L., et al. “ASMBS allied health nutritional guidelines for the surgical weight loss patient.” *Surgery for Obesity and Related Diseases* 4.5 (2008): S73-S108.
- Varban, O. A., et al. “Differences in operative outcomes between Roux-en-Y gastric bypass and sleeve gastrectomy in older adults.” *JAMA Surgery* 150.12 (2015): 1139-1145.
- Courcoulas, A. P., et al. “Long-term outcomes of bariatric surgery: a National Institutes of Health symposium.” *JAMA surgery* 149.12 (2014): 1323-1329.
- Mechanick, J. I., et al. “Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update.” *Surgery for Obesity and Related Diseases* 9.2 (2013): 159-191.

Trackbacks and Pingbacks